Appendix B. Toxicity Assessment Overview
Toxicity values for many chemicals have been developed by USEPA and other regulatory or public health agencies (for example, ATSDR, WHO). As a result, in the process of conducting a risk assessmentAn organized process used to describe and estimate the likelihood of adverse health outcomes from environmental exposures to chemicals. The four steps are hazard identification, dose-response assessment, exposure assessment, and risk characterization (Commission 1997a)., a risk assessor is generally not charged with the task of conducting toxicity assessments. More often, toxicity valuesDerived values (for example, reference doses and slope factors) that can be used to estimate the incidence or potential for adverse human health effects in receptor (USEPA 2015h). for most if not all chemicals of potential concern at a site are available from readily accessible sources.
The risk assessor should, however, understand the basis, assumptions, and uncertainties that underlie the derivation of toxicity values. This understanding can help appropriately characterize and communicate the risks from a particular exposure scenarioA set of facts, data, assumptions, and professional judgment about how an exposure occurs or does not occur. An exposure scenario addresses the (1) chemicals in environmental media and their sources; (2) exposed populations (or receptors); (3) migration of chemicals in environmental media from sources to receptors; and (4) routes of exposure (ingestion, dermal contact, inhalation). and assist risk managers in making informed risk managementThe process of identifying, evaluating, selecting, and implementing actions to reduce risk to human health and to ecosystems. The goal of risk management is scientifically sound, cost-effective, integrated actions that reduce or prevent risks while taking into account social, cultural, ethical, political, and legal considerations (Commission 1997a). decisions.
Toxicity values have many descriptors and qualifiers: cancer and noncancer, oral and inhalation, and chronic, subchronic, and acute. The toxicity values used to evaluate a particular exposure scenario should be consistent with the calculation being performed (cancer risk versus noncancer risk), the exposure routes of interested (oral, dermal contact, inhalation) and, in the case of noncancer risk, the exposureContact of a receptor with a chemical. Exposure is quantified as the amount of the chemical available at the exchange boundaries of the organism (for example, skin, lungs, gut) and available for absorption (USEPA 1989a). period being evaluated (chronic, subchronic, or acute exposure).
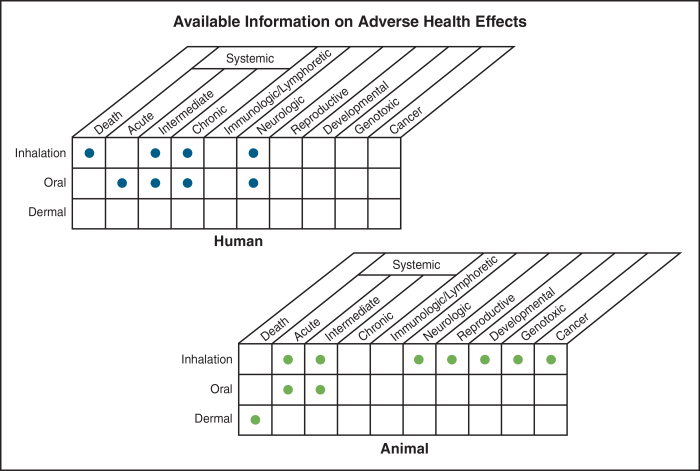
Figure B-1. Consideration of adverse effect (endpoint), route of exposure, and relevance to human health in toxicity assessmentThe combination of the hazard identification and the dose response assessment..
Source: Figure 3-4 of ATSDR 2006.
The toxicity assessment component of a risk assessment considers the types of adverse health effects associated with chemical exposures (Figure B-1), the relationship between the magnitude of exposure and adverse effects (Figure B-2), and related uncertainties such as the weight of evidence of a particular chemical’s carcinogenicity in humans (USEPA 1989a).
The toxicity assessment commonly involves two steps: hazard identificationThe process of determining whether exposure to a chemical in environmental media by a receptor can cause an increase in the incidence of an adverse human health effect (for example, incremental lifetime cancer risk) (USEPA 2012b). and dose-response assessmentThe relationship between exposure level (amount of chemical in an environmental media that is inhaled, absorbed, or ingested by a receptor) and the incidence of adverse effects (adapted from Commission 1997a). (USEPA 2012c). Figure B-2 illustrates multiple adverse health effects and related dose response relationships for the same chemical. The outcome of a toxicity assessment is usually expressed as a toxicity value, such as a reference dose (RfD)A dose specified by USEPA to limit human oral and dermal exposure to potentially hazardous levels of chemicals that are thought to have thresholds for their effects, such as noncarcinogens (Commission 1997a). or cancer slope factorAn upper bound, approximating a 95% confidence limit, on the increased cancer risk from a lifetime exposure to an agent. This estimate, usually expressed in units of proportion (of a population) affected per mg/kg-day, is generally reserved for use in the low-dose region of the dose-response relationship, that is, for exposures corresponding to risks less than 1 in 100 (USEPA 2013). (CSF), which incorporates the findings of the hazard and dose-response assessments and safety factors that address uncertainties in the assessment. A toxicity assessment may also conclude that a toxicity value cannot be developed because of inadequate data.
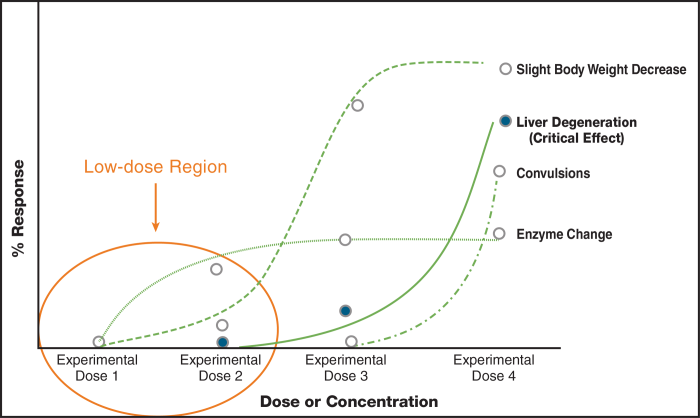
Figure B-2. Multiple adverse health effects and related dose-response relationships for the same chemical.
Source: NCEA, USEPA (USEPA 2010b).
B.1 Toxicity Assessment of Noncarcinogens
Chemicals with known or assumed noncancer effects are presumed to have a dose below which no adverse effects occur, because of the body’s ability to eliminate or detoxify the chemical. The dose at which this effect occurs is known as the threshold dose. In laboratory experiments, the highest nonzero tested dose at which no adverse effects occur is called the “no observed adverse effect level” (NOAEL) and the lowest dose where an adverse effect does occur is known as the “lowest observed adverse effect level” (LOAEL). The threshold dose in the experimental model lies between the NOAEL and LOAEL. The value of the NOAEL and LOAEL depends on the design of the experiment: an experiment with more or fewer animals, or with a difference selection of test doses, will have a different NOAEL and LOAEL. Some toxicity studies fail to identify a NOAEL as a result of dose selection or lack of statistical significance in increased effect (Figure B-4).
The benchmark dose (BMD) corresponding to a lower limit of a one-sided 95% confidence interval on the BMD, is USEPA’s preferred approach to using NOAEL/LOAEL approach because it is determined using all data from a dose-response curve and is not limited by dose selection. (Figure B-3) The BMD is selected as the dose level that produces a predetermined change in adverse response. With a degree of certainty, noncancer effects are not expected to occur if the dose is below the threshold, regardless if the exposure occurs daily for the span of a lifetime. Figure B-4 illustrates how points of departure within individual toxicity studies can differ.
Noncancer toxicity values are in units of milligrams of compound per kilogram of body weight (mg/kg-day) for oral/dermal exposure and micrograms of compound per meter cubed of inhaled air (µg/m3) for inhalation exposure.
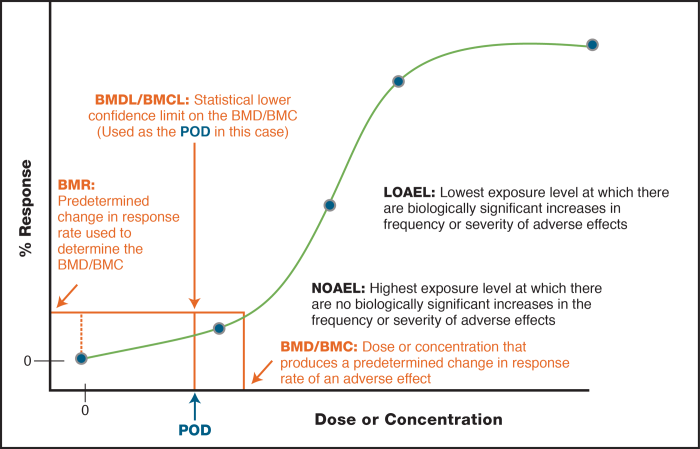
Figure B-3. Dose-response curve showing various options for points of departure for a noncancer endpoint.
Source: NCEA, USEPA (USEPA 2010b).
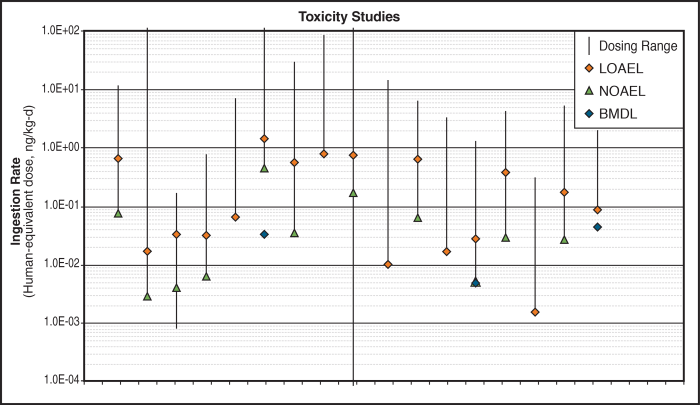
Figure B-4. Comparison of points of departure derived across studies for various adverse effects from same chemical. More than an order of magnitude difference in possible points of departure within studies is shown, with implications for reference value determination.
Source: NCEA, USEPA (USEPA 2010b).
Typically, animal dose-response toxicity studies provide data for hazard identification and toxicity values. This approach presents an uncertaintyThe lack of perfect knowledge of values or parameters used in a risk assessment. Uncertainty may be reduced by collection of additional data. or knowledge gap in comparing how humans might respond relative to the animals models used. To account for this uncertainty, USEPA and other agencies apply uncertainty factors (UFs) when an oral reference dose (RfD) or inhalation reference concentration (RfC)A concentration specified by USEPA to limit human inhalation exposure to potentially hazardous levels of chemicals in air (Commission 1997a). is derived from animal studies. The RfD/RfC value is derived by dividing the point of departure (NOAEL, LOAEL or BMD) by the overall UFs. The UFs are generally applied, when appropriate, to account for:
- the uncertainty in extrapolating from the LOAEL in the absence of the NOAEL;
- the use of the NOEL obtained from a subchronic study an extrapolating to a chronic exposure;
- confidence in the adequacy of the overall database;
- interspecies extrapolation (animal to human);
- intra-species variation in sensitivity.
Application of UFs to a study’s point of departure is intended to produce a health-protective estimate of threshold that is lower than the actual threshold.
B.2 Toxicity Assessment of Carcinogens
For chemicals with known or assumed cancer effects, it is typically presumed in the absence of sufficient evidence that no threshold dose for effects exists (in other words, some incremental level of risk is associated with any dose above zero). To assess carcinogenic effects, a two-step process is used. First, a chemical is assigned a weight-of-evidence classification based on the likelihood that a chemical is a human carcinogen (for example, “known”, “probable”, “suggestive evidence”). If the chemical drives the risk estimate at a site, then this classification may factor into a site management decision, such as response urgency.
Next, if a chemical is a known or probable human carcinogen, then a CSF is calculated. Various models may be used to calculate the CSF, but all assume that there is no threshold and use both animal and human data to calculate the CSF, with a 95% upper confidence bound on the slope (the actual unit risk is likely lower); see Figure B-5. The CSF is expressed as the rate of cancer per unit of dose (mg/kg-day)-1 or as an inhalation unit risk factor (IUR) as the rate of cancer per unit of concentration of inhaled air (µg/m3).
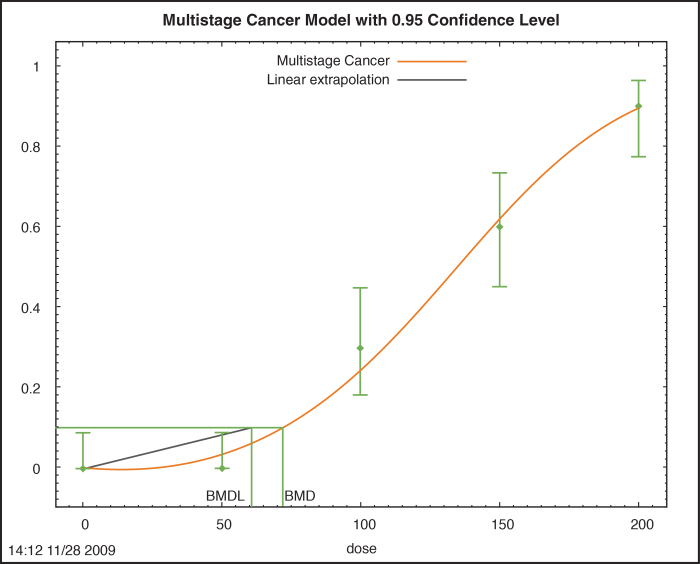
Figure B-5. Determination of a cancer slope factor.
Source: Environ, used with permission.
B.3 Summary
Toxicity assessment of chemicals entails its own practices of accounting for uncertainty to generate values adequately protective of human health in risk management informed by risk assessment. These practices include assumptions made regarding the potential for health effects in humans based on animal studies, as well as adoption of uncertainty factors and upper confidence limits to quantify reference values and potency factors. The criteria for chemicals of concern at sites change as new toxicity studies become relevant and adequate or improved data quality becomes available. Risk managers must be aware of these issues and how they may affect decision making in risk management and communication. Alternatively, a toxicologist should be included on the project team for support regarding these issues.
B.4 Additional Resources
USEPA provides general guidance for conducting cancer and noncancer risk assessments, including the development and review of reference and risk values for health effects in humans. The following resources were not cited in the sections above and are included here for further information.
USEPA Cancer Guidelines (USEPA 2005b)
USEPA RfC Guidelines (USEPA 1994b)
Review of RfD and RfC Derivation Process (USEPA 2002d)
USEPA Science Policy Council Guidelines (USEPA 2000b) and (USEPA 2015b)
National Center for Environmental Assessment Guidelines for Peer Review (NCEA 2009)
NIH Introduction to Toxicology and Dose-Response (NIH 2010)
Publication Date: January 2015